Female Urogyneacology
Stress Urinary incontinence is a common problem in later age. We have done successfully bladder neck & mid urethral suspension surgery by T-Suit, TOT - Transobturotor mid urethral sling surgery. Other patient can be treated medically.
We do cystoscopy, uroflowmetry & complete urodynamics workup for patient of voiding difficulties.
We treat patient of recurrent UTI.
Advantages of TOT :
- Day care procedure
- Minimally invasive
- Nearly painless
- Durable
Urinary incontinence is an inability to hold your urine until you get to a toilet. More than 13 million people in the United States male and female, young and old experience incontinence. It is often temporary, and it always results from an underlying medical condition.
(In this fact sheet, the term "incontinence" will be used to mean urinary incontinence.)
Women experience incontinence twice as often as men. Pregnancy and childbirth, menopause, and the structure of the female urinary tract account for this difference. But both women and men can become incontinent from neurologic injury, birth defects, strokes, multiple sclerosis, and physicalproblems associated with aging.
Older women, more often than younger women, experience incontinence. But incontinence is not inevitable with age. Incontinence is treatable and often curable at all ages. If you experience incontinence, you may feel embarrassed. It may help you to remember that loss of bladder control can be treated. You will need to overcome your embarrassment and see a doctor to learn if you need treatment for an underlying medical condition.
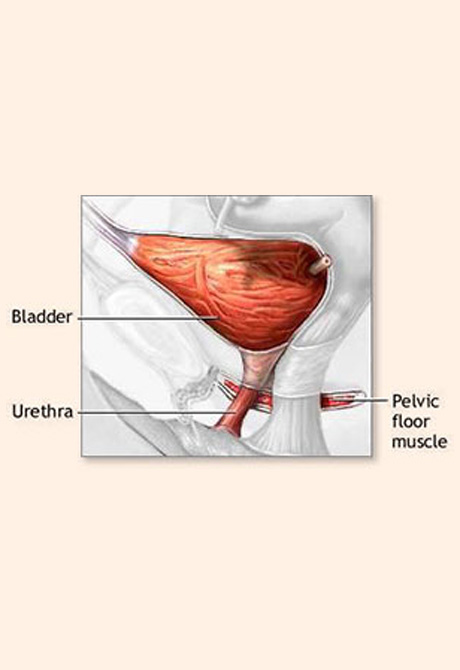
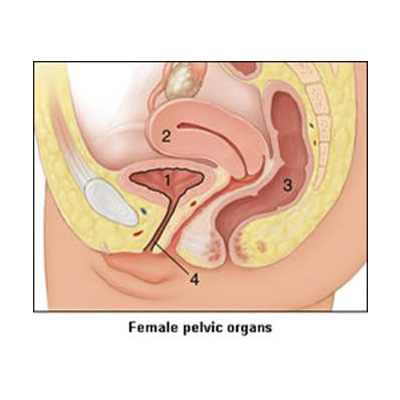
Incontinence in women usually occurs because of problems with muscles that help to hold or release urine. The body stores urine water and wastes removed by the kidneys in the bladder, a balloon-like organ. The bladder connects to the urethra, the tube through which urine leaves the body.
During urination, muscles in the wall of the bladder contract, forcing urine out of the bladder and into the urethra. At the same time, sphincter muscles surrounding the urethra relax, letting urine pass out of the body. Incontinence will occur if your bladder muscles suddenly contract or muscles surrounding the urethra suddenly relax.
Stress Incontinence
If coughing, laughing, sneezing, or other movements that put pressure on the bladder cause you to leak urine, you may have stress incontinence. Physical changes resulting from pregnancy, childbirth, and menopause often cause stress incontinence. It is the most common form of incontinence in women and is treatable.
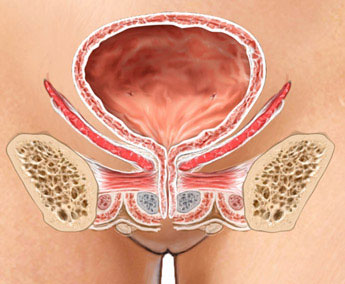
Pelvic floor muscles support your bladder. If these muscles weaken, your bladder can move downward, pushing slightly out of the bottom of the pelvis toward the vagina. This prevents muscles that ordinarily force the urethra shut from squeezing as tightly as they should. As a result, urine can leak into the urethra during moments of physical stress. Stress incontinence also occurs if the muscles that do the squeezing weaken.
Stress incontinence can worsen during the week before your menstrual period. At that time, lowered estrogen levels might lead to lower muscular pressure around the urethra, increasing chances of leakage. The incidence of stress incontinence increases following menopause.
The Types of Urinary Incontinence
Stress- Leakage of small amounts of urine during physical movement (coughing, sneezing, exercising).
Urge- Leakage of large amounts of urine at unexpected times, including during sleep.
Functional - Untimely urination because of physical disability, external obstacles, or problems in thinking or communicating that prevent a person from reaching a toilet.
Overflow- Unexpected leakage of small amounts of urine because of a full bladder.
Mixed- Usually the occurrence of stress and urge incontinence together.
Transient- Leakage that occurs temporarily because of a condition that will pass (infection, medication).
How is Incontinence evaluated?
The first step toward relief is to see a doctor who is well acquainted with incontinence to learn what type you have. A urologist specializes in the urinary tract, and some urologists further specialize in the female urinary tract. Gynecologists and obstetricians specialize in the female reproductive tract and childbirth. A urogynecologist focuses on urological problems in women. Family practitioners and internists see patients for all kinds of complaints. Any of these doctors may be able to help you.
To diagnose the problem, your doctor will first ask about symptoms and medical history. Your pattern of voiding and urine leakage may suggest the type of incontinence. Other obvious factors that can help define the problem include straining and discomfort, use of drugs, recent surgery, and illness. If your medical history does not define the problem, it will at least suggest which tests are needed.
Your doctor will physically examine you for signs of medical conditions causing incontinence, such as tumors that block the urinary tract, stool impaction, and poor reflexes or sensations, which may be evidence of a nerve-related cause. Your doctor will measure your bladder capacity and residual urine for evidence of poorly functioning bladder muscles. To do this, you will drink plenty of fluids and urinate into a measuring pan, after which the doctor will measure any urine remaining in the bladder. Your doctor may also recommend.
Stress test. You relax, then cough vigorously as the doctor watches for loss of urine.
Urinalysis Urine is tested for evidence of infection, urinary stones, or other contributing causes.
Blood tests Blood is taken, sent to a laboratory, and examined for substances related to causes of incontinence.
Ultrasound Sound waves are used to "see" the kidneys, ureters, bladder, and urethra. Cystoscopy A thin tube with a tiny camera is inserted in the urethra and used to see the inside of the urethra and bladder.
Your doctor may ask you to keep a diary for a day or more, up to a week, to record when you void. This diary should note the times you urinate and the amounts of urine you produce. To measure your urine, you can use a special pan that fits over the toilet rim.
How is incontinence treated?
Exercises Kegel exercises to strengthen or retrain pelvic floor muscles and sphincter muscles can reduce or cure stress leakage. Women of all ages can learn and practice these exercises, which are taught by a health care professional. Most Kegel exercises do not require equipment. However, one technique involves the use of weighted cones. For this exercise, you stand and hold a cone-shaped object within your vagina. You then substitute cones of increasing weight to strengthen the muscles that help keep the urethra closed.
Electrical Stimulation Brief doses of electrical stimulation can strengthen muscles in the lower pelvis in a way similar to exercising the muscles. Electrodes are temporarily placed in the vagina or rectum to stimulate nearby muscles. This will stabilize overactive muscles and stimulate contraction of urethral muscles. Electrical stimulation can be used to reduce both stress incontinence and urge incontinence.
Bio feedback uses measuring devices to help you become aware of your body's functioning. By using electronic devices or diaries to track when your bladder and urethral muscles contract, you can gain control over these muscles. Biofeedback can be used with pelvic muscle exercises and electrical stimulation to relieve stress and urge incontinence.
Timed Voiding or Bladder Training Timed voiding (urinating) and bladder training are techniques that use biofeedback. In timed voiding, you fill in a chart of voiding and leaking. From the patterns that appear in your chart, you can plan to empty your bladder before you would otherwise leak. Biofeedback and muscle conditioning known as bladder training can alter the bladder's schedule for storing and emptying urine. These techniques are effective for urge and overflow incontinence. Medications: Medications can reduce many types of leakage. Some drugs inhibit contractions of an overactive bladder. Others relax muscles, leading to more complete bladder emptying during urination. Some drugs tighten muscles at the bladder neck and urethra, preventing leakage. And some, especially hormones such as estrogen, are believed to cause muscles involved in urination to function normally. Some of these medications can produce harmful side effects if used for long periods. In particular, estrogen therapy has been associated with an increased risk for cancers of the breast and endometrium (lining of the uterus). Talk to your doctor about the risks and benefits of long-term use of medications.
Pessaries A pessary is a stiff ring that is inserted by a doctor or nurse into the vagina, where it presses against the wall of the vagina and the nearby urethra. The pressure helps reposition the urethra, leading to less stress leakage. If you use a pessary, you should watch for possible vaginal and urinary tract infections and see your doctor regularly.
Implants are substances injected into tissues around the urethra. The implant adds bulk and helps to close the urethra to reduce stress incontinence. Collagen (a fibrous natural tissue from cows) and fat from the patient's body have been used. Implants can be injected by a doctor in about half an hour using local anesthesia. Implants have a partial success rate. Injections must be repeated after a time because the body slowly eliminates the substances. Before you receive collagen, a doctor must perform a skin test to determine whether you would have an allergic reaction to the material.
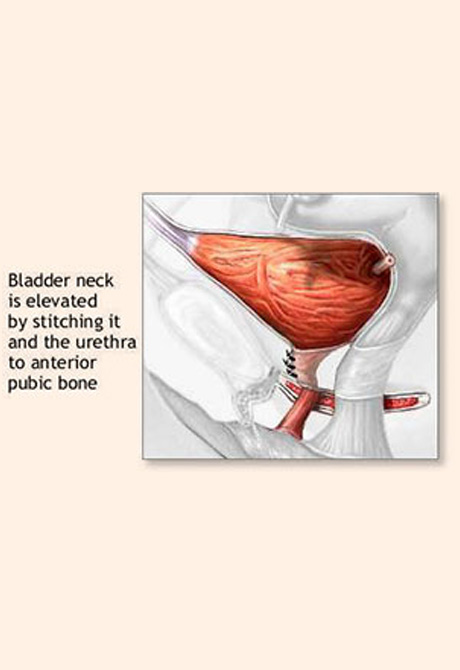
Surgery Doctors usually suggest surgery to alleviate incontinence only after other treatments have been tried. Many surgical options have high rates of success. Most stress incontinence results from the bladder dropping down toward the vagina. Therefore, common surgery for stress incontinence involves pulling the bladder up to a more normal position. Working through an incision in the vagina or abdomen, the surgeon raises the bladder and secures it with a string attached to muscle, ligament, or bone. For severe cases of stress incontinence, the surgeon may secure the bladder with a wide sling. This not only holds up the bladder but also compresses the bottom of the bladder and the top of the urethra, further preventing leakage. In rare cases, a surgeon implants an artificial sphincter, a doughnut-shaped sac that circles the urethra. A fluid fills and expands the sac, which squeezes the urethra closed. By pressing a valve implanted under the skin, you can cause the artificial sphincter to deflate. This removes pressure from the urethra, allowing urine from the bladder to pass.
Catheterization If you are incontinent because your bladder never empties completely (overflow incontinence) or your bladder cannot empty because of poor muscle tone, past surgery, or spinal cord injury, you might use a catheter to empty your bladder. A catheter is a tube that you can learn to insert through the urethra into the bladder to drain urine. Catheters may be used once in a while or on a constant basis, in which case the tube connects to a bag that you can attach to your leg. If you use a long-term (or indwelling) catheter, you should watch for possible urinary tract infections.
Other Procedures
Many women manage urinary incontinence with pads that catch slight leakage during activities such as exercising. Also, you often can reduce incontinence by restricting certain liquids, such as coffee, tea, and alcohol. Finally, many women who could be treated resort instead to wearing absorbent undergarments, or diapers�especially elderly women in nursing homes. This is unfortunate, because diapering can lead to diminished self-esteem, as well as skin irritation and sores. If you are an elderly woman, you and your family should discuss with your doctor the possible effectiveness of treatments such as timed voiding, pelvic muscle exercises, and electrical stimulation before resorting to absorbent pads or undergarments.